|
SENSORY PATHWAYS
Sensory pathways include only those routes which
conduct information to the conscious cortex of the brain.
However, we will use the term in its more
loosely and commonly applied context to include input from all
receptors, whether their signals reach the conscious level or
not.
 GENERAL
SOMATIC AFFERENT (GSA) PATHWAYS FROM THE BODY
GENERAL
SOMATIC AFFERENT (GSA) PATHWAYS FROM THE BODY
 Pain and
Temperature
Pain and
Temperature
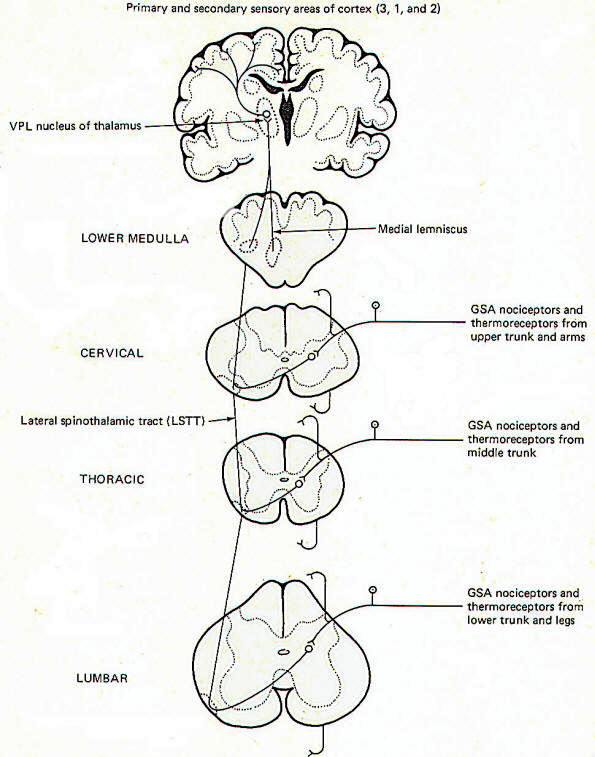
Pain and
temperature information from general somatic receptors is
conducted over small-diameter (type A delta and type C) GSA
fibers of the spinal nerves into the posterior horn of the
spinal cord gray matter (Fig-1). These are monopolar neurons
with cell bodies in the posterior root ganglia. After entering
the cord, the fibers pass up or down in the dorsolateral
tract, located between the tip of the posterior horn and the
surface of the spinal cord near the posterior root, before
finally synapsing in laminae III and IV.
 |
|
| Fig-1 |
|
Second-order neurons from these synapses cross over to the
opposite side of the cord in the anterior white commissure,
where they turn upward as the lateral spinothalamic tract (LSTT).
At higher pontine levels this tract comes to lie close to the
medial lemniscus, with which it travels to the ventral posterior
lateral nucleus (VPL) of the thalamus. Some fibers of this tract
don't enter the thalamus but end instead in the brainstem
reticular formation. After synapsing in the thalamus,
third-order neurons enter the posterior third of the internal
capsule, pass through the corona radiata, and terminate in the
primary and secondary sensory areas of the parietal lobe cortex
(areas 3,1, and 2). Notice that regardless of the level of entry
into the spinal cord, pain and temperature stimulation
delivered to one side of the body registers in the cerebral
cortex of the opposite side.
Fast and
Slow Pain
Pain sensation is often confusingly labeled "fast" or
"slow" depending on the type of fiber which conducts the impulse
and the speed with which the signal consciously registers. Fast
pain, often called sharp or pricking pain, is usually conducted
to the CNS over type A delta fibers. These ultimately excite
lateral spinothalamic tract fibers which go directly to the VPL
of the thalamus on the contralateral side. From here third-order
fibers project to the cerebral cortex where they are
somatotopically organized and sharply localized. Somatotopic
organization means that each minute area of the sensory cortex
receives input from a distinct peripheral area. A person can
sharply localize a pain if he is able to tell exactly where it
is originating. Slow pain, often called burning pain, is
conducted to the CNS over smaller-diameter type C fibers. After
entering the cord these fibers stimulate lateral spinothalamic
tract neurons which send collaterals into the brainstem
reticular formation. Fibers from the reticular formation
diffusely project to the thalamus, hypothalamus, and possibly
other areas as well, perhaps giving rise to the emotional
component of pain. Pain signals following this route are poorly
localized.
Dermatomes
A dermatome is the area of skin supplied by the afferent fibers
in the posterior root of a single spinal nerve. Dermatomes tend
to overlap each other so that stimulation of a specific point on
the skin typically sends afferent signals into the cord over
more than one posterior root. This is functionally important
since destruction of a single posterior root does not totally
eliminate sensation from the afflicted dermatome.
Touch and
Pressure
Touch can
be subjectively described as discriminating or crude.
Discriminating (epicritic) touch implies an awareness of an
object's shape, texture, three-dimensional qualities, and other
fine points. Also implied here is the ability to recognize
familiar objects simply by tactile manipulation. Crude (protopathic)
touch, on the other hand, lacks the fine discrimination
described above and doesn't generally give enough information to
the brain to enable it to recognize a familiar object by touch
alone. The tactile information implied here is of a much cruder
nature than described for epicritic touch. The pathways to the
brain for these two kinds of touch appear to be distinct.
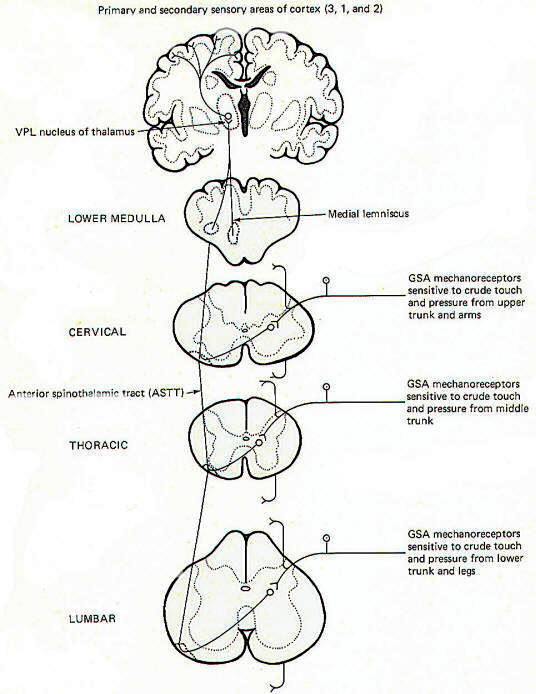
Crude (Protopathic)
Touch and Pressure
General somatic mechanoreceptors sensitive
to crude touch and pressure conduct information into the cord
over GSA nerve fibers (Fig-2). The fibers pass up or down a
few cord segments (neuromeres) in the dorsolateral (Lissauer)
tract before synapsing chiefly in laminae VI, VII, and VIII.
Second-order neurons cross over to the opposite side in the
anterior white commissure to the anterior funiculus, where they
turn upward in the anterior spinothalamic tract (ASTT) to the
VPL of the thalamus. At higher pontine levels the tract also
comes to lie close to the medial lemniscus as it ascends to the
thalamus. Third-order neurons project from the VPL to areas 3,
1, and 2 of the cerebral cortex. Some of the ASTT fibers send
collaterals into the brainstem reticular formation. While some
of these no doubt ultimately reach the thalamus by
reticulothalamic projections, the principal fate and function of
these collaterals is largely unknown.
 |
|
| Fig-2 |
|
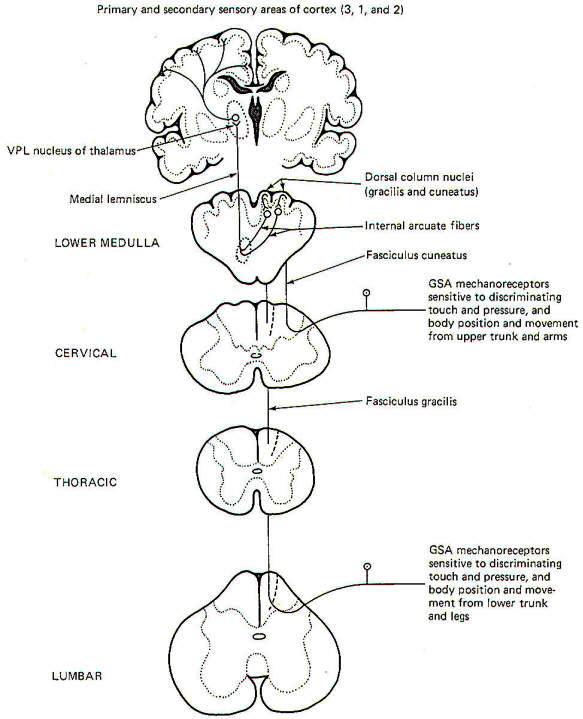
Discriminating (Epicritic) Touch, Pressure, and Kinesthesia
The
conscious awareness of body position and movement is called the
kinesthetic sense. It's important to recognize that there are
many receptors throughout the body which continually conduct
information to the brain concerning the body's position and
movement and even the level of muscle tone. Such receptors are
collectively called proprioceptors. However, not all of these
signals reach the conscious level as a large portion are
conducted instead to the brainstem and cerebellum for
subconscious evaluation and integration. Only those
proprioceptive signals reaching the conscious level contribute
to the kinesthetic sense. The kinesthetic sense and
discriminating touch and pressure pathways share a common route
to the brain (Fig-3).
 |
|
| Fig-3 |
|
General
somatic mechanoreceptors sensitive to discriminating touch and
pressure and body position and movement conduct signals into the
cord over GSA fibers. They pass directly into the ipsilateral
posterior funiculus, where they turn upward in the dorsal
columns to terminate in the dorsal column nuclei of the medulla.
Those fibers entering the cord below the midthoracic level
(i.e., from the lower trunk and legs) ascend through the medial
dorsal column as the fasciculus gracilis and terminate in the
nucleus gracilis. Fibers entering the cord above the midthoracic
level (i.e., from the upper trunk and arms) enter the more
lateral dorsal column and ascend as the fasciculus cuneatus to
terminate in the more lateral dorsal column nuclei, the nucleus
cuneatus. As might be expected, the dorsal columns include the
fasciculus gracilis and fasciculus cuneatus while the dorsal
column nuclei include the nucleus gracilis and nucleus cuneatus.
Second-order neurons from these nuclei cross over to the other
side of the brainstem in the lower medulla as the internal
arcuate fibers. which then turn upward in the medial lemniscus
to the VPL of the thalamus. Third-order neurons then project
through the posterior limb of the internal capsule to areas 3,
1, and 2 of the cerebral cortex.
Much of the
proprioceptive information which reaches the conscious level
giving rise to the kinesthetic sense originates in joint
receptors. However, recent evidence indicates that signals from
muscle spindles may also represent a significant contribution to
kinesthetic sensation. On the other hand, the subconscious
proprioceptive information which is shunted to the brainstem and
cerebellum for evaluation and integration arises chiefly in
muscle spindles and Golgi tendon organs.
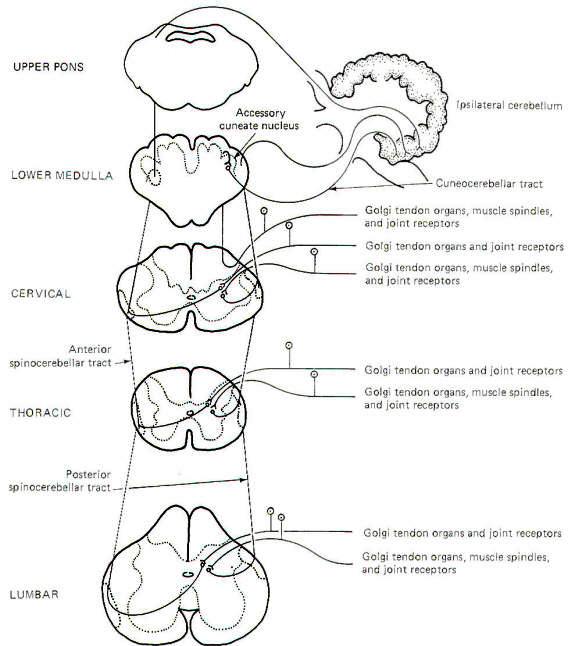
Subconscious Proprioception
Most of the
subconscious proprioceptive input is shunted to the cerebellum.
Further, signals arising in proprioceptors on the left side of
the body register on the left side of the cerebellum. By
contrast, sensory signals arising in the left side of the body
register on the right side of the cerebral cortex. After
entering the cord, proprioceptive afferents (GSA fibers)
terminate in laminae V, VI, and VII (Clarke's column) of the
posterior horn. Second-order neurons (primarily conducting
information from Golgi tendon organs) cross over to the opposite
side of the cord in the anterior white commissure to the lateral
funiculus, where they turn upward in the anterior
spinocerebellar tract (ASCT). After reaching upper pontine
levels the fibers cross back over and enter the cerebellum
through the superior cerebellar peduncle, where they terminate
in the vermis (Fig-4). Some of the anterior spinocerebellar
tract fibers upon reaching the medulla remain uncrossed and
enter the cerebellum via the inferior cerebellar peduncle and
terminate in the contralateral vermis. Other second-order
neurons (those receiving information primarily from muscle
spindles and tendon organs) leave Clarke's
column to ascend in the ipsilateral posterior spinocerebellar
tract (PSCT) to the cerebellum. After reaching the medulla, the
fibers enter the cerebellum via the inferior cerebellar
peduncle to terminate in the ipsilateral cortex.
 |
|
| Fig-4 |
|
Some of the
subconscious proprioceptive input from the cervical region
follows an alternate route to the cerebellum. Some of the fibers
travel a short distance in the dorsal funiculus, terminating in
the accessory cuneate nucleus of the medulla. Second-order
neurons project from here as the cuneocerebellar tract to enter
the cerebellum via the inferior cerebellar peduncle.
Posterior
Funiculus Injury
Certain clinical signs are associated with
injury to the dorsal columns. As might be expected, these are
generally caused by impairment to the kinesthetic sense and
discriminating touch and pressure pathways. They include (1) the
inability to recognize limb position, (2) astereognosis, (3)
loss of two-point discrimination, (4) loss of vibratory sense,
and (5) a positive Romberg sign. Astereognosis is the inability
to recognize familiar objects by touch alone. When asked to
stand erect with feet together and eyes closed, a person with
dorsal column damage may sway and fall. This is a positive
Romberg sign.
GENERAL
SOMATIC AFFERENT (GSA) PATHWAYS FROM THE FACE
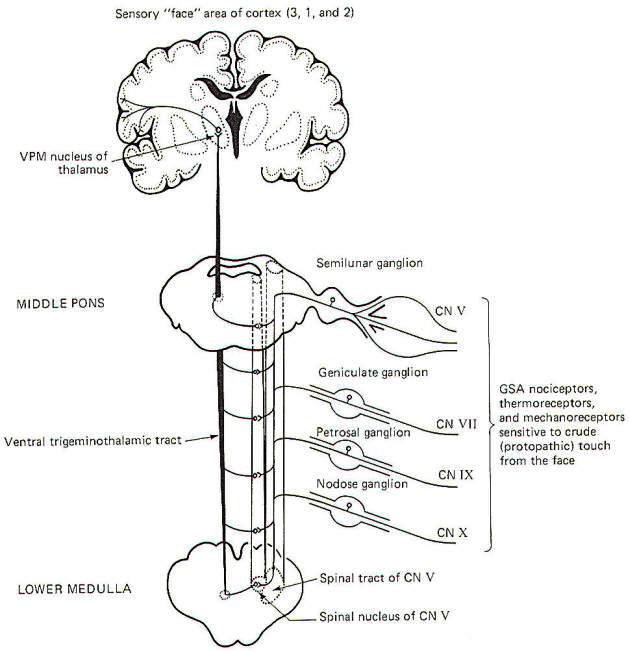
Pain,
Temperature, and Crude Touch and Pressure
General
somatic nociceptors, thermoreceptors, and mechanoreceptors
sensitive to crude touch and pressure from the face conduct
signals to the brainstem over GSA fibers of cranial nerves V,
VII, IX, and X. The afferent fibers involved are processes of
monopolar neurons with cell bodies in the semilunar,
geniculate, petrosal, and nodose ganglia, respectively. The
central processes of these neurons enter the spinal tract of V,
where they descend through the brainstem for a short distance
before terminating in the spinal nucleus of V. Second-order
neurons then cross over the opposite side of the brainstem at
various levels to enter the ventral trigeminothalamic tract,
where they ascend to the VPM of the thalamus. Finally,
third-order neurons project to the "face" area of the cerebral
cortex in areas 3, 1, and 2 (Fig-5).
 |
| Fig-5 |
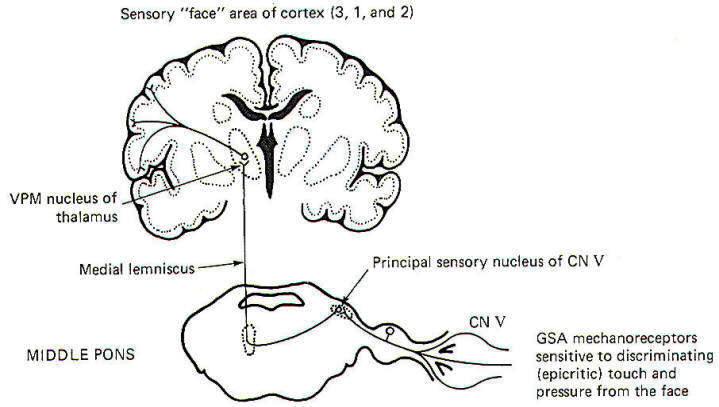
Discriminating Touch and Pressure
The pathway
for discriminating touch from the face is illustrated in Fig-6. Signals are conducted from general somatic mechanoreceptors
over GSA fibers of the trigeminal nerve into the principal
sensory nucleus of V, located in the middle pons. Second-order
neurons then conduct the signals to the opposite side of the
brainstem, where they ascend in the medial lemniscus to the VPM
of the thalamus. Thalamic neurons then project to the "face"
region of areas 3, I, and 2 of the cerebral cortex.
 |
| Fig-6 |
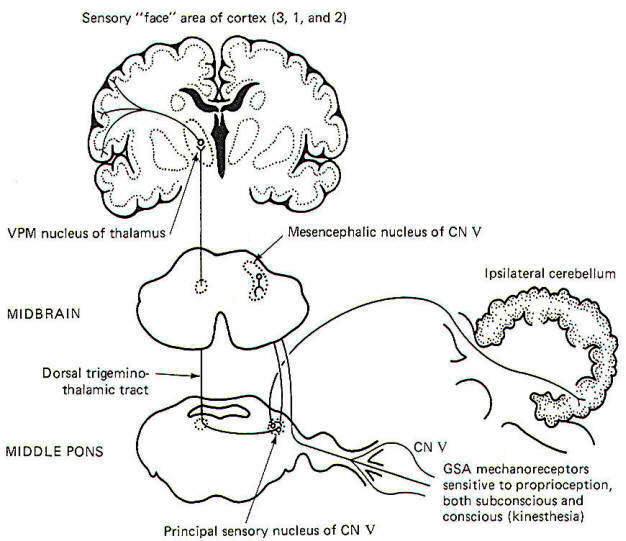
Kinesthesia
and Subconscious Proprioception
Proprioceptive input from the face is primarily conducted over
GSA fibers of the trigeminal nerve. Curiously, however, the cell
bodies of these monopolar neurons are located in the
mesencephalic nucleus of V in the midbrain rather than the
semilunar ganglia, where the cell bodies of other afferent
neurons of the trigeminal nerve are located. The peripheral
endings of these neurons are the general somatic
mechanoreceptors sensitive to both conscious (kinesthetic) and
subconscious proprioceptive input. Their central processes
extend from the mesencephalic nucleus to the principal sensory
nucleus of V in the pons (Fig-7).
 |
| Fig-7 |
The
subconscious component is conducted to the cerebellum, while the
conscious component travels to the cerebral cortex. Certain
second-order neurons from the principal sensory nucleus relay
proprioceptive information concerning subconscious evaluation
and integration into the ipsilateral cerebellum. Other
second-order neurons project to the opposite side of the pons
and ascend to the VPM of the thalamus as the dorsal trigeminothalamic tract. Thalamic projections terminate in the
face area of the cerebral cortex.
SPECIAL
SOMATIC AFFERENT (SSA) PATHWAYS
|
 Hearing
Hearing
The organ
of Corti with its sound-sensitive hair cells and basilar
membrane are important parts of the sound transducing system for
hearing. Mechanical vibrations of the basilar membrane generate
membrane potentials in the hair cells which produce impulse
patterns in the cochlear portion of the vestibulocochlear nerve
(VIII). The principles of this system will be examined
elsewhere. For now we will examine only the central pathways from the
receptors to their terminations in the brain (Fig-8).
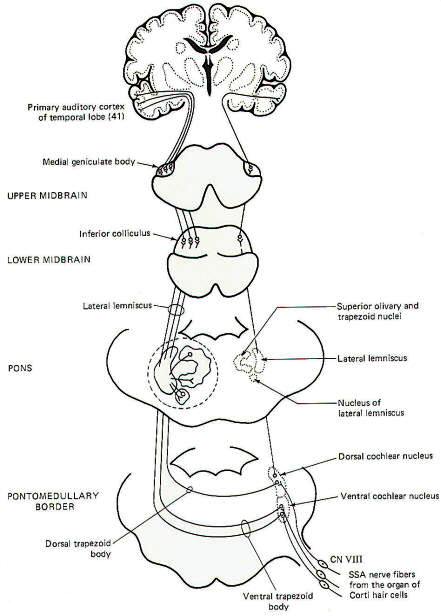
Special
somatic nerve fibers of cranial nerve VIII relay impulses from
the sound receptors (hair cells) in the cochlear nuclei of the
brainstem. These are bipolar neurons with cell bodies located in
the spiral ganglia of the cochlea. Their central processes
terminate in the dorsal and ventral cochlear nuclei on the
ipsilateral side of the brain stem at the pontomedullary border.
Most of the second-order neurons arising in the cochlear nuclei
cross to the opposite side of the brainstem in the trapezoid
body and turn upward in the lateral lemniscus, terminating in
the inferior colliculus of the midbrain. Collaterals of the
lateral lemniscus terminate in the nucleus of the trapezoid
body, superior olivary nucleus, nucleus of the lateral
lemniscus, and the brainstem reticular formation. Fibers arising
in these nuclei also ascend in the lateral lemniscus. Those
fibers from the cochlear nuclei which don't cross over in the
trapezoid body ascend in the ipsilateral lateral lemniscus to
the inferior colliculus. Sound signals also pass from one side
to the other via contralateral projections from one lemniscal
nucleus to the other as well as from one inferior colliculus to
the other. Thus each lateral lemniscus conducts information from
both sides, which helps to explain why damage to a lateral
lemniscus produces no appreciable hearing loss other than
problems with sound localization. Signals are then conducted
from the inferior colliculi to the medial geniculate bodies and
finally to the primary auditory area of the temporal lobes (area
41). |
 |
| Fig-8 |
Vestibular
System
The
vestibulocochlear nerve serves two quite different functions.
The cochlear portion, previously described, conducts sound
information to the brain, while the vestibular portion conducts
proprioceptive information. It is the central neural pathways of
the latter function which we will examine now (Fig-9). The
mechanics and physiology of the system explained
elsewhere.
 |
| Fig-9 |
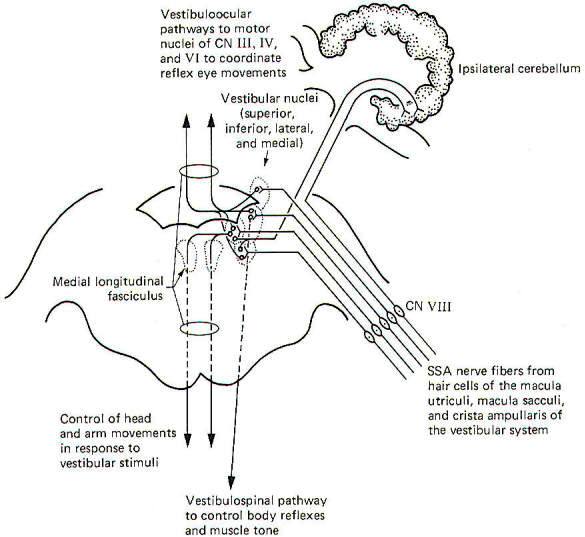
Special
somatic afferent fibers from the hair cells of the macula
utriculi and macula sacculi conduct information into the
vestibular nuclei on the ipsilateral side of the pons and
medulla. These are bipolar neurons with cell bodies located in
the vestibular ganglion. Some of the fibers project directly
into the ipsilateral cerebellum to terminate in the uvula,
flocculus, and nodulus, but most enter
the vestibular nuclei and synapse there.
As might be
expected, neuronal output from the vestibular nuclei effects
bodily and eye movements in response to movements of the head as
detected by the vestibular apparatus. The vestibulospinal path
fibers which affect body reflexes and muscle tone in response to
vestibular input originate primarily in the lateral vestibular
nucleus. The medial vestibular nucleus is the principal origin
of both crossed and uncrossed fibers which descend through the
brain stem in the medial longitudinal fasciculus to the upper
cord causing various reflex head and arm movements in response
to vestibular stimuli. Finally, all four vestibular nuclei
(medial, lateral, superior, and inferior) project both crossed
and uncrossed fibers to the motor nuclei of cranial nerves Ill,
IV, and VI in order to control and coordinate reflex eye
movements. These vestibuloocular paths also travel in the medial
longitudinal fasciculus.
Vision
The visual
system receptors are the rods and cones of the retina. The neurophysiology of vision
and visual reflexes are discussed
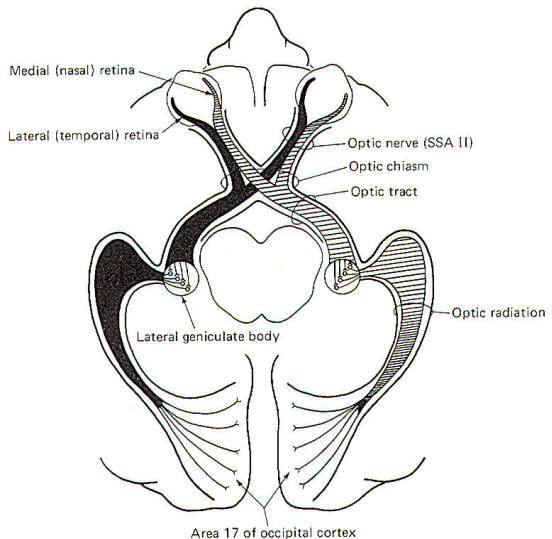
elsewhere. Special
somatic afferent fibers of the optic nerve (II) conduct visual
signals into the brain. Examination of Fig-10 will show that
fibers from the lateral (temporal) retina of either eye
terminate in the lateral geniculate body on the same side of the
brain as that eye. On the other hand, SSA II fibers from the
medial (nasal) retina of each eye cross over in the optic chiasm
to terminate in the contralateral lateral geniculate body. The
optic nerve is composed of fibers from the retina to the optic
chiasm. Even though no synapses occur in the optic chiasm, the
continuation of the visual pathway from the optic chiasm to the
lateral geniculate body is called the optic tract rather than
the optic nerve. After a synapse in the lateral geniculate body,
the signal continues in the optic radiation to area 17 of the
conscious visual cortex. Area 17 is the primary visual area,
which receives initial visual signals. Neurons from this area
project into the adjacent occipital cortex (areas 18 and 19)
which is known as the secondary visual area. It is here that the
visual signal is fully evaluated.
 |
 |
| Fig-10 |
Fig-11 |
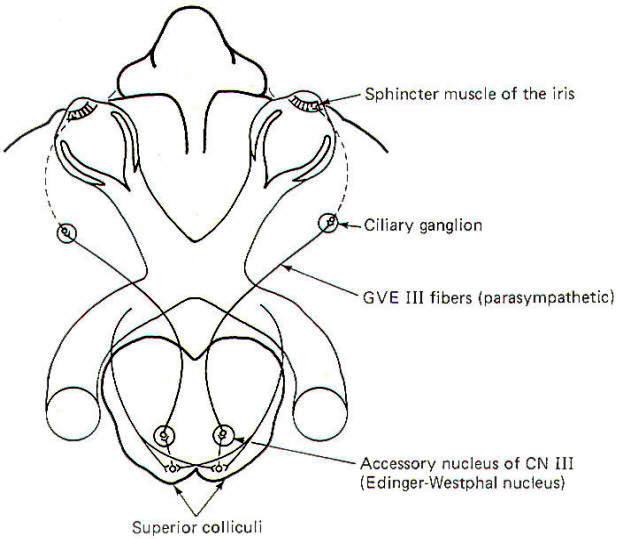
The visual
reflex pathway involving the pupillary light reflex is
illustrated in Fig-11. This is the well-known reflex in which
the pupils constrict when a light is shined into the eyes and
dilate when the light is removed. Some SSA II fibers leave the
optic tract before reaching the lateral geniculates, terminating
in the superior colliculi instead. From here, short neurons
project to the EdingerWestphal nucleus (an accessory nucleus of
III) in the midbrain, which serves as the origin of the
preganglionic parasympathetic fibers of the oculomotor nerve
(GVE III). The GVE III fibers in turn project to the ciliary
ganglia, from which arise the postganglionic fibers to the
sphincter muscles of the iris, which constrict the pupils.
GENERAL
VISCERAL AFFERENT (GVA) PATHWAYS
Pain and Pressure Sensation via
the Spinal Cord
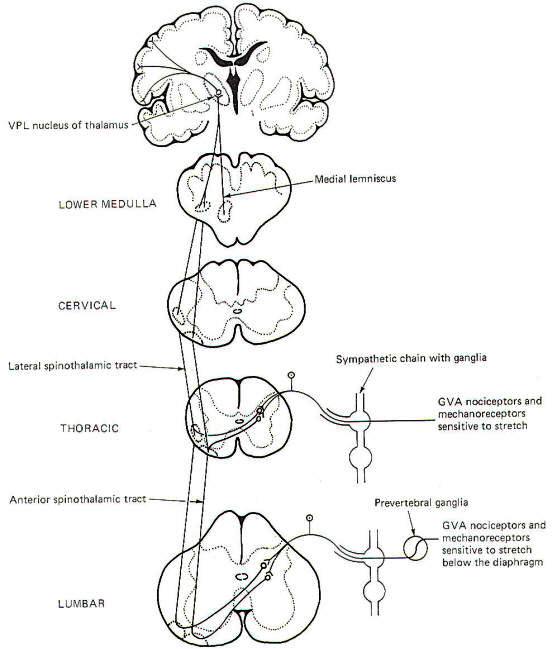
Visceral
pain receptors are located in peritoneal surfaces, pleural
membranes, the dura mater, walls of arteries, and the walls of
the GI tube. Nociceptors in the walls of the GI tube are
particularly sensitive to stretch and overdistension.
General
visceral nociceptors conduct signals into the spinal cord over
the monopolar neurons of the posterior root ganglia. They
terminate in laminae III and IV of the posterior horn as do the
pain and temperature pathways of the GSA system; however, their
peripheral processes reach the visceral receptors via the gray
rami communicantes and ganglia of the sympathetic chain (Fig12), Second-order neurons from the posterior horn cross in the
anterior white commissure and ascend to the thalamus in the
anterior and lateral spinothalamic tracts, Projections from the
VPL of the thalamus relay signals to the sensory cortex.
 |
 |
| Fig-12 |
Fig-13 |
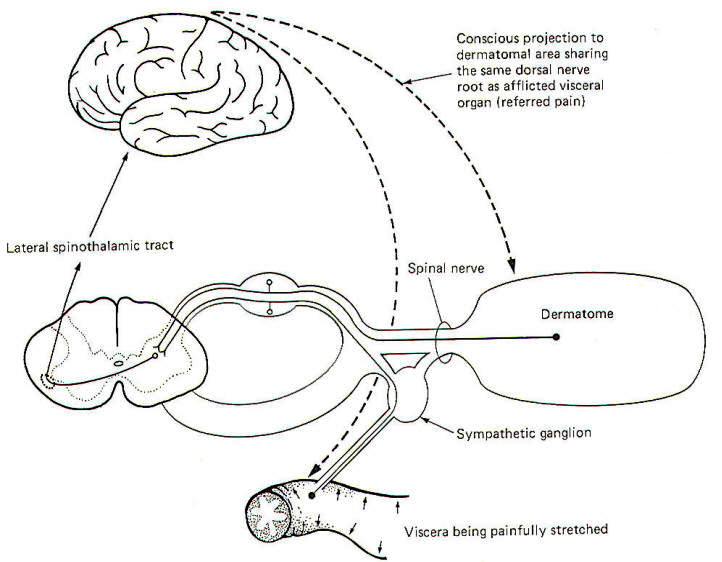
The
localization of visceral pain is relatively poor, making it
difficult to tell the exact source of the stimuli. At least a
partial explanation of our inability to precisely localize
visceral pain relates to its rarity. True visceral pain seldom
occurs when compared to the frequency of external pain. An
additional compounding factor is the phenomena of referred
pain. Because true visceral pain is often projected or
"referred" by the brain to some area on the surface of the body,
its true visceral origin is often confused. The mechanism for
referred visceral pain is not fully understood but may result
in part from the close proximity in the posterior horn of the
central terminals of GVA pain fibers and GSA spinal nerve
fibers from the body surface. This is supported by the fact that
pain from a visceral origin is referred to a dermatome with
which it shares the same posterior root. This is a useful
observation, often making it possible to locate the source of a
visceral pain from an observation of the surface area to which
it is referred. The pain down the inside of the left arm
associated with true cardiac pain is a good example.
It is
likely that separate second-order neurons relay pain information
from GSA and GVA input. If the painful stimulus to the viscera
is moderate, the level of activity in the GVA fibers is likely
sufficient to stimulate only those second-order neurons which
normally relay signals from the viscera. However, if the painful
stimulus increases in strength, the increased central synaptic
activity of the GVA neurons may "spill over" and raise the
central excitatory state of those second-order neurons which
normally relay information from GSA fibers of the dermatome. If
the painful visceral stimulation is very strong, this "spill
over" may be sufficient to exceed the threshold of excitation
for these neurons, causing them to fire even though no painful
stimulus is delivered to the general somatic nociceptors of the
dermatome. Thus the brain incorrectly projects the source of
the pain to the dermatomal area (Fig-13).
|
Blood
Pressure, Blood Chemistry, and Alveolar Stretch Detection
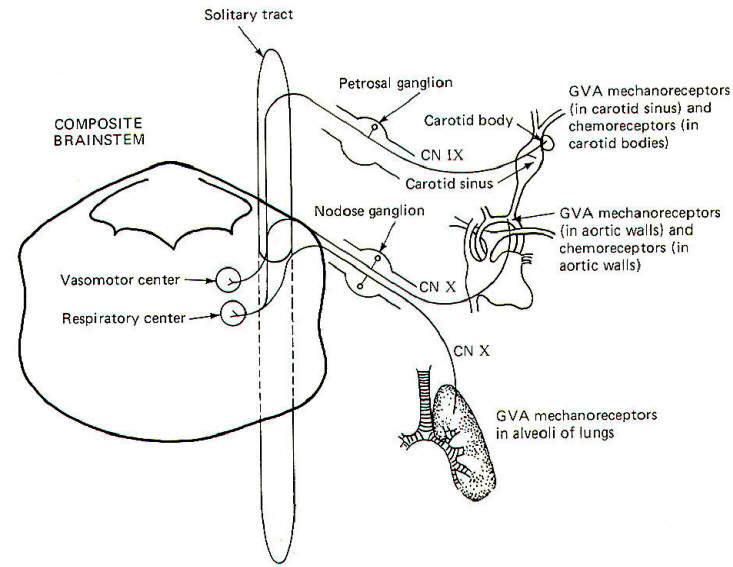
The walls
of the aorta and the carotid sinuses contain special
baroreceptors (pressure receptors) which respond to changes in
blood pressure. These mechanoreceptors are the peripheral
endings of GVA fibers of the glossopharyngeal (IX) and vagus
(X) nerves. The GVA fibers from the carotid sinus
baroreceptors enter the solitary tract of the brainstem and
terminate in the vasomotor center of the medulla (Fig-14).
This is the CNS control center for cardiovascular activity. The
cell bodies of these unipolar neurons are located in the
petrosal ganglion. GVA fibers of the vagus nerve conduct
signals from the baroreceptors in the walls of the aorta to the
solitary tract and on to the vasomotor center. The cell bodies
of these unipolar neurons are located in the nodose ganglion.
Stretch
receptors in the alveoli of the lungs conduct information
concerning rhythmic alveolar inflation and deflation over GVA
X fibers to the solitary tract and then to the respiratory
center of the brainstem. This route is an important link in the Hering-Breuer reflex, which helps to regulate respiration.
Carotid
body chemoreceptors, sensitive to changes in blood PO2 and, to a
lesser extent, PCO2 and pH, conduct signals to both the
vasomotor and respiratory centers over GVA IX nerve fibers. GVA X fibers conduct similar information from the aortic
chemoreceptors to both centers. Chemoreceptors were discussed
elsewhere.
|
 |
| Fig-14 |
SPECIAL
VISCERAL AFFERENT (SVA) PATHWAYS
Taste
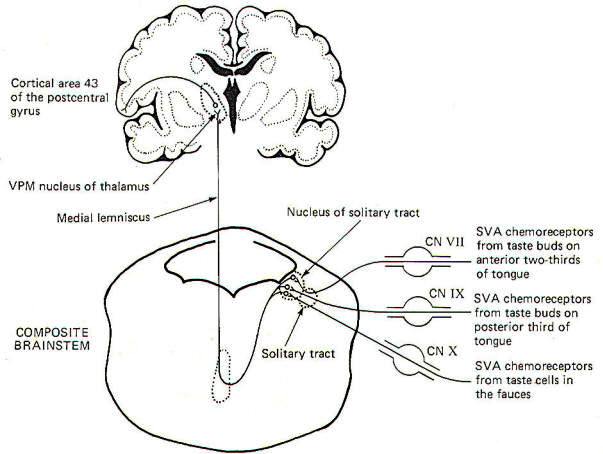
The
receptors for taste are the taste cells which produce impulses
in afferent fibers in response to chemical stimulation. They
were described elsewhere. The pathways for taste sensation are
illustrated in Fig-15. Special
visceral afferent (SVA) fibers of cranial nerves VII, IX, and X
conduct signals into the solitary tract of the brainstem,
ultimately terminating in the nucleus of the solitary tract on
the ipsilateral side. Second-order neurons cross over and ascend
through the brainstem in the medial lemniscus to the VPM of the
thalamus. Thalamic projections to area 43 (the primary taste
area) of the postcentral gyrus complete the relay. SVA VII
fibers conduct from the chemoreceptors of taste buds on the
anterior twothirds of the tongue, while SVA IX
fibers conduct taste information from buds on the posterior
one-third of the tongue. SVA X fibers conduct taste signals
from those taste cells located throughout the fauces.
 |
 |
| Fig-15 |
Fig-16 |
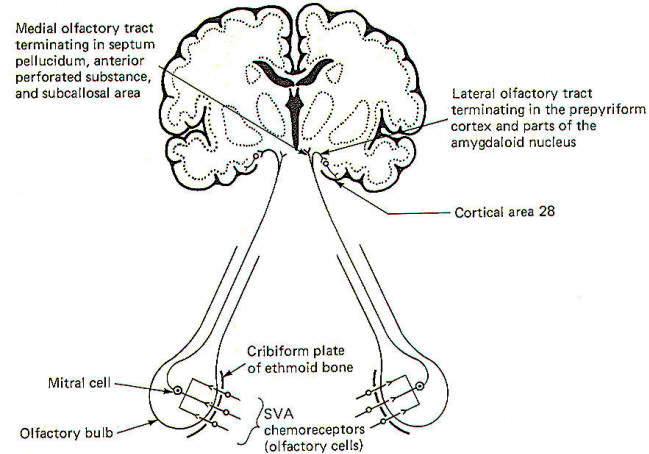
Smell
The sense
of smell was examined
elsewhere and, once again, we will look
only at the central pathways here. The smell-sensitive cells
(olfactory cells) of the olfactory epithelium project their
central processes through the cribiform plate of the ethmoid
bone, where they synapse with mitral cells. The central
processes of the mitral cells pass from the olfactory bulb
through the olfactory tract, which divides into a medial and
lateral portion (Fig-16). The lateral olfactory tract
terminates in the prepyriform cortex and parts of the amygdala
of the temporal lobe. These areas represent the primary
olfactory cortex. Fibers then project from here to area 28, the
secondary olfactory area, for sensory evaluation. The medial
olfactory tract projects to the anterior perforated substance,
the septum pellucidum, the subcallosal area, and even the
contralateral olfactory tract. Both the medial and lateral
olfactory tracts contribute to the visceral reflex pathways,
causing the viscerosomatic and viscerovisceral responses
described earlier.
 DAMAGE TO
THE SPINAL NERVES AND SPINAL CORD
DAMAGE TO
THE SPINAL NERVES AND SPINAL CORD
After
studying the motor pathways and the sensory pathways, the
injuries described in Table-1 would be expected to produce the
symptoms listed.
|
Table-1 Symptoms of Damage to Spinal Nerves and Spinal
Cord |
|
Damage |
Possible cause of damage |
Symptoms associated with innervated
area |
|
Peripheral nerve |
Mechanical injury |
Loss of muscle tone. Loss of
reflexes. Flaccid paralysis. Denervation atrophy.
Loss of sensation |
|
Posterior root |
Tabes dorsalis |
Paresthesia. Intermittent sharp
pains. Decreased sensitivity to pain. Loss of reflexes. Loss of
sensation. Positive
Romberg sign. High
stepping and slapping of feet. |
|
Anterior
Horn |
Poliomyelitis |
Loss of muscle
tone. Loss of reflexes. Flaccid paralysis. Denervation atrophy |
|
Lamina X (gray
matter) |
Syringomyelia |
Bilateral loss of pain and
temperature sense only at afflicted cord level.
Sensory dissociation. No
sensory impairment below afflicted level |
|
Anterior horn and
lateral corticospinal tract |
Amyotrophic
lateral sclerosis |
Muscle weakness. Muscle
atrophy. Fasciculations of hand and arm muscles. Spastic
paralysis |
|
Posterior and lateral funiculi |
Subacute combined degeneration |
Loss of position sense. Loss of
vibratory sense. Positive Romberg sign.
Muscle weakness. Spasticity.
Hyperactive tendon reflexes. Positive Babinski sign. |
|
Hemisection of the spinal cord |
Mechanical injury |
Brown-Sequard syndrome |
|
Below cord level
on injured
side |
|
Flaccid paralysis.
Hyperactive tendon reflexes. Loss of
position sense. Loss of vibratory sense. Tactile impairment |
|
Below cord level on opposite side beginning one or
two segments below injury |
|
Loss
of
pain and
temperature |
|